278-005 DBS Trial Going For Surgery Next Wednesday

The operation is Wednesday. Patient 005 is having a deep brain stimulation device implanted on Wednesday, give him some support, here: DBS Trial
The operation is Wednesday. Patient 005 is having a deep brain stimulation device implanted on Wednesday, give him some support, here: DBS Trial
In Deep Brain Stimulation for treatment resistant depression with stimulation of Broadman area 25 (Cg 25) no consistent declines in memory for either verbal or visual material were noted after onset or maintenance of DBS over baseline. This makes DBS a procedure with out apparent cognitive side effects in treatment resistant depression. In a recent publication with DBS in the Subthalamic Nucleus for treatment resistant Obsessive Compulsive Disorder (OCD) no cognitive decline was found. The ratings of neuropsychological measures were not modified by stimulation.

In 17 patients participating in this 10-month, crossover, double-blind, multicenter study assessing the efficacy and safety of stimulation of the subthalamic nucleus one patient had a parenchymal brain hemorrhage (bleeding) resulting in a permanent finger palsy. Two patients had an infection leading to removal of the pulse generator. Seven transient motor and psychiatric symptoms induced by active stimulation occurred in the first month of stimulation and resolved spontaneously or rapidly after adjustment of the setting. Ten other patients also had serious but transient side-effects.Three patients became hypomanic, three suffered from anxiety, two of depressive symptomps the others suffered from transient neurological side-effects such as dyskinesia, trouble walking, dysarthria, dysphagia and facial asymmetry.
Deep Brain Stimulation of the subthalamic nucleus significantly reduced the symptoms of severe forms of OCD.
In conclusion, findings from this 3-month crossover study suggest that stimulation of the subthalamic nucleus may lessen the severity of obsessive–compulsive symptoms and improve global functioning in patients with refractory, severe OCD. Serious adverse events occurred in 11 of the 17 patients in whom stimulators were implanted. The occurrence of severe adverse events, the small number of patients, and the short duration of the study highlight the risks of stimulation of the subthalamic nucleus and the need for larger studies with longer follow-up. In addition to assessment in a larger number of patients, a comparison with other stimulation targets and surgical procedures would be desirable, as would an evaluation of the long-term benefits of stimulation of the subthalamic nucleus in patients with OCD, notably with respect to their quality of life and their ability to function in social and work environments.

Read a review on the use of deep brain stimulation (DBS). Wrote a lot of posts about this new treatment on this blog, mostly for treatment resistant depression. As with most new treatment options the new treatment is tried with other severe diseases. You can probably find some on this blog or down this post in the related posts section. The use of DBS in Alzheimer’s disease drew my attention. Stimulating certain brain regions in a disease with a neurodegenerative character seems almost impossible.
This review was written by members of the Canadian group who also published about the use of DBS in treatment resistant depression. They stimulated certain brain regions serving cognitive and memory functions (the fornix, part of the Papez memory circuit) in six patients with Alzheimer’s disease.
After 1 year of chronic high-frequency stimulation, glucose hypometabolism within the temporoparietal cortex that is characteristic of the diseased brain was largely reversed
Two patients improved on the Mini Mental State Examination, three others declined and one was unchanged. The average decline on points of the MMSE suggest a delay of this cognitive decline for these patients.
It was just a pilot study and needs further research. The authors have started a large multicenter trial
J. Schouenborg, M. Garwicz and N. Danielsen (Eds.)
Progress in Brain Research, Vol. 194
Deep brain stimulation: emerging indications
Travis S. Tierney, Tejas Sankar and Andres M. Lozano
New long term data on efficacy of deep brain stimulation for treatment resistant depression are available. The first follow up data up to 1 year were already promising. Published research about deep brain stimulation for treatment resistant depression showed that six months after surgery, 60% of patients were responders and 35% met criteria for remission, benefits that were largely maintained at 12 months.
The average response rate to DBS after two and three years were 46,2% and 75%. More than one-third of patients were in remission at year 3. But what’s more convincing functional impairment in the areas of physical health and social functioning progressively improved up to the last follow-up visit.
The Mayberg group published a follow up for 6 patients after 6 months and they subsequently reported on 12 month outcomes in an expanded sample of 20 patients. The last report at 3 years of follow-up as summarized above were also with 20 patients. The report on the extended follow-up of these 20 patients results from data from 3 to 6 years (mean=3.5 years) after DBS implantation. The mean duration of follow-up of the 20 patients was 42,1 months. In general patients required less medication after DBS implantation.
Adverse events
Two patients died by suicide during depressive relapses. This is of concern but stipulates the severity of the illness and it’s consequences. From the editorial:
One issue arising from this study requires special attention—that of suicide. Two of the 20 patients in this extended follow-up study committed suicide, and two others made suicide attempts. There is no evidence suggesting that DBS was related to these deaths. Rather, these suicides reflect the severity and seriousness of treatment resistant depression. In one of these patients there had been periods of sustained remission, but the patient relapsed and required a course of ECT prior to her suicide. The other patient had persistent suicidal ideation. These results underscore the high mortality in patients with treatment-resistant depression, even with careful and frequent monitoring by experienced and competent providers. It should serve as an impetus for us to continue to strive to develop new strategies to treat this patient population.
The first year three of the first six patients had hardware infections, no device related adverse events occurred after those three. Eight battery replacement surgeries were required during follow-up (mean time to battery replacement, 43.3 months).
Over the course of follow-up, eight patients were hospitalized for medical reasons on a total of 12 occasions. Half of these admissions were for psychiatric reasons (worsening depression, N=3; suicidal ideation, N=3), and the other half were for nonpsychiatric reasons
Other scarce reports on efficacy and follow up with DBS targeting other areas also show comparable results. Limitations of this study:
Open label, selected group of nonpsychotic unipolar depressed patients which leaves it unclear whether other forms of depression will also respond favorably.
![]()
Kennedy SH, Giacobbe P, Rizvi SJ, Placenza FM, Nishikawa Y, Mayberg HS, & Lozano AM (2011). Deep brain stimulation for treatment-resistant depression: follow-up after 3 to 6 years. The American journal of psychiatry, 168 (5), 502-10 PMID: 21285143
Hirschfeld RM (2011). Deep brain stimulation for treatment-resistant depression. The American journal of psychiatry, 168 (5), 455-6 PMID: 21536698

According to this neurosurgeon, the strongest evidence exists for Broadman Area 25 in the subcallosal cingulate gyrus (SCG) as target for deep brain stimulation in treatment resistant depression.. This area in the brain is depicted in the figure above and is from the most important publication about DBS and depression in Neuron march 2005 by Helen Mayberg. Functional neuroimaging as well as antidepressant treatment effects suggest that this area plays an important role in modulating negative mood states. A decrease in activity is reported with clinical response to antidepressants and electroconvulsive therapy (ECT).
But depression is not a disease of a single brain region nor neurotransmitter system. It is now generally viewed as a systems-level disorder affecting integrated pathways linking select cortical, subcortical, and limbic brain regions with their related neurotransmitter systems.
Suggestions of other brain localizations for treatment with DBS for depression comes from case reports with DBS for other indications than depression. These localizations have been described in a peer reviewed article with excelent graphics.
In a recent study done by the “Mayberg group”, Toronto, Canada, the autors compared the location of the electrode contacts in responders and nonresponders to DBS of the subcallosal cingulate gyrus (SCG) and correlated the results with clinical outcome to help in identifying the optimal target within the region.

On postoperative MRI scans the researchers did complicated mapping procedures to pin point the locations of the active contacts on the implanted electrodes. There was no difference when the right and left electrodes were compared in patients. So both electrodes were exactly placed on each side (hemisphere). The only significant difference they found between responders and nonresponders was that electrodes in patients who responded were in a slightly more ventral position relative to the anatomical landmarks used in the medial prefrontal lobe. This difference between responders and nonresponders did not exceed 1,5 mm. The authors is not likely to be of clinical significance, according to the authors. This small difference is probably unimportant compared to the clinical features of the patient for the outcome of the DBS procedure in depression. Another limiting factor on this research is the small sample size, in larger groups these results might differ.
What we can conclude based on our findings is that within the small targeted region of the SCG, the location of the electrode contacts did not determine outcome.
This article also describes a detailed method for a more standardized method for targeting the SCG with DBS for depression. This is to technical to reproduce in this post but those working with DBS for depression should have a look at this procedure. From this study it is still not clear whether DBS of other brain areas might be more superior in efficacy. And is brain area more important than clinical features of the patient or do the areas differ for different types of depression? All very interesting questions and topic for more research on DBS.
![]()
Hamani, C., Mayberg, H., Snyder, B., Giacobbe, P., Kennedy, S., & Lozano, A. (2009). Deep brain stimulation of the subcallosal cingulate gyrus for depression: anatomical location of active contacts in clinical responders and a suggested guideline for targeting Journal of Neurosurgery, 111 (6), 1209-1215 DOI: 10.3171/2008.10.JNS08763
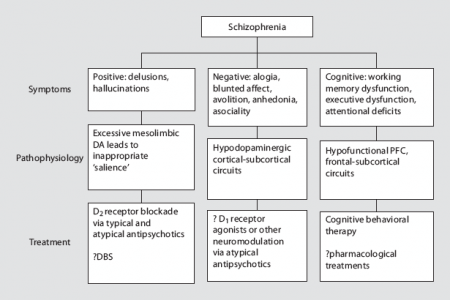
In short, a recent article proposed to do deep brain stimulation for schizophenia. Schizophrenia has positive-, negative- and cognitive symptoms (see the figure above). The authors propose the DBS for positive symptoms. Their approach is based on current models of the neurocircuitry of psychosis .
They hypothesize:
that chronic, high frequency electrical stimulation (HFS) of the hippocampus or the nucleus accumbens (NAc), through stabilization of dopamine (DA) release in the striatum, may improve positive symptoms in patients with schizophrenia.
I checked Clinicaltrials.gov but no one is doing a trial with DBS and schizophrenia yet.
Their hypothesis is based on the assumption that hippocampal hyperactivity early in the course of the illness leads to excessive dopamine release and the appearance of positive symptoms. Stimulation of the hippocampus might slow down this hyper stimulation as in a rodent model of schizophrenia.
The nucleus accumbens plays an important part in the dopamine release in response to hippocampal activation, stimulation of the nucleus accumbens might interrupt this circuit and stabilize dopamine release.

In their article they also propose other possible targets but the above mentioned are their favorites. They conclude with the suggestion that their hypotheses needs to be verified with neuroimaging and animal models.
Finally, our claim that stabilization of DA levels is the most likely explanation for the clinical effects of NAc stimulation needs to be evaluated experimentally. A variety of human, nonhuman primate, and rodent studies using in vivo microdialysis, micro-PET, and other techniques could be designed for this purpose.
What do you think will there be a place for deep brain stimulation for schizophrenia?
In the accompanying comment questions are raised whether the dopamine model is not to simple. Other neurotransmitters also play a role in schizophrenia. Moreover, stimulating the hippocampus might also affect cognition and emotions. The chief complaint being the wide range of phenotypes with schizophrenia. We don’t even know whether schizophrenia is just one disease or the face of many. And what about negative symptoms. They won’t be lessened according to this hypotheses. Nevertheless an interesting read.
![]()
Mikell, C., McKhann, G., Segal, S., McGovern, R., Wallenstein, M., & Moore, H. (2009). The Hippocampus and Nucleus Accumbens as Potential Therapeutic Targets for Neurosurgical Intervention in Schizophrenia Stereotactic and Functional Neurosurgery, 87 (4), 256-265 DOI: 10.1159/000225979
Bakay, R. (2009). Deep Brain Stimulation for Schizophrenia Stereotactic and Functional Neurosurgery, 87 (4), 266-266 DOI: 10.1159/000225980

In a recent online publication about another form of brain stimulation in treatment resistant depression showed promising results. The electrodes are placed on the brain instead of in the brain as with Deep Brain Stimulation (DBS):
A new neurosurgical procedure may prove helpful for patients with treatment-resistant depression. Bilateral epidural prefrontal cortical stimulation (EpCS) was found generally safe and provided significant improvement of depressive symptoms in a small group of patients
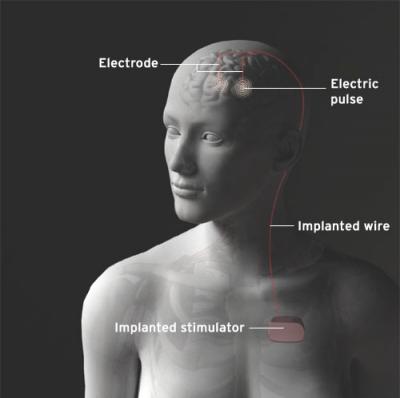
The location for Brain Stimulation in EpCS targets electrical stimulation to the anterior frontal poles and the lateral prefrontal cortex. Two different places on both hemispheres, resulting in four separate paddle leads which are connected to two small generators surgically implanted in the upper chest area of the patient. The leads are placed through a burr hole in the skull but above the dura mater and thus remain separated from the underlying cortical region by the arachnoid space. ECS is more direct than transcranial magnetic stimulation (TMS) and or vagus nerve stimulation (VNS) and potentially safer than deep brain stimulation (DBS), which involves passing the electrodes through brain tissue.
Of five patients three reached remission. Overall after seven months, the average improvement was 54.9 percent based on the Hamilton Rating Scare for Depression.
Advantages according to the team:
“Cortical stimulation has several advantages provided that it shows efficacy in treating depression. It is reversible, non-destructive and potentially safer than other forms of invasive brain stimulation since the stimulating paddles don’t come in direct contact with the brain.”
Deep Brain Stimulation is a neuro-surgical procedure used in mostly neurological and psychiatric disorders. In this procedure electrodes are placed in the brain, not on the brain. A great step forward, patients don’t have to be awake during the procedure. This post has a video showing a clear description of the old and new procedure for deep brain stimulation (DBS).
Deep Brain Stimulation (DBS) is mostly used for Parkinson’s Disease. DBS for Obsessive Compulsive Disorder and Depression is just starting to be used. It is unclear how DBS works for Parkinson’s Disease.
It is used for treatment resistant depression. When other treatments fail, deep-brain stimulation (DBS) may offer hope to patients suffering from chronic and severe depression. In recent published research about deep brain stimulation for treatment resistant depression, six months after surgery, 60% of patients were responders and 35% met criteria for remission, benefits that were largely maintained at 12 months.
The most appropriate target, optimal stimulation parameters, and long-term effects and efficacy remain uncertain. The targets for deep brain stimulation in treatment resistant depression has 6 options available.
![]()
![]()
Nahas, Z., Anderson, B., Borckardt, J., Arana, A., George, M., Reeves, S., & Takacs, I. (2009). Bilateral Epidural Prefrontal Cortical Stimulation for Treatment-Resistant Depression Biological Psychiatry DOI: 10.1016/j.biopsych.2009.08.021
A great step forward, patients don’t have to be awake during the procedure. This video shows a clear description of the old and new procedure for deep brain stimulation (DBS). In the old procedure a frame has to applied after which a brain mapping procedure has to follow, up to 6-8 hours while the patient has to be awake. At the end the patient has to undergo a MRI to see whether the electrodes are in the right place. All very tedious and time consuming. The new procedure takes place in the MRI with anesthesia and takes less time (50%). Have a look at this new procedure in the video.
Is there new hope for Parkinson’s patients? Imaging scientist, Alastair Martin, and neurosurgeon, Dr. Paul Larson, have teamed up to develop a way to perform Deep Brain Stimulation surgery that’s more comfortable for the patients, more accurate and cuts the regular procedure time in half to 3 1/2 hours. The pair, working at the University of California in San Francisco perform DBI surgery while the patient is inside the MRI . The advantage to the procedure is that the patient does not have to be awake, it detects complications on the spot and allows for precise placement of the electrodes in the brain.
Thanks Smartplanet
More recent news on deep brain stimulation on New Scientist: Smart implants may alleviate neurological conditions
SMART implants in the brains of people with neurological disorders could eventually help develop treatments for people with Parkinson’s disease, depression and obsessive compulsive disorder.
Related posts on this blog:
These ethical guidelines were recently published in the JAMA and I fully agree with these guidelines. The article starts with a brief description of DBS, it’s complications and a short history of the lessons from past errors of psychosurgery.
Important lessons from the abuses of psychosurgery in the last century make it imperative to have solid hypotheses with strong scientific support and appropriate safeguards (eg, interdisciplinary review boards) before proceeding to treat patients using DBS.
Using these guidelines with the recent technological advances DBS can perhaps help a lot of patients in the near future.
![]()
Kringelbach, M., & Aziz, T. (2009). Deep Brain Stimulation: Avoiding the Errors of Psychosurgery JAMA: The Journal of the American Medical Association, 301 (16), 1705-1707 DOI: 10.1001/jama.2009.551
Alleviating Parkinsons through deep brain stimulation from Science News on Vimeo.
Deep Brain Stimulation (DBS) is mostly used for Parkinson’s Disease. DBS for Obsessive Compulsive Disorder and Depression is just starting to be used. It is unclear how DBS works for Parkinson’s Disease. With DBS an electrical probe is inserted into the brain and it stimulates an area known as the subthalamic nucleus. This can help people with Parkinson’s disease overcome the disorder’s neurological block on movement.
But how does this stimulation work. Some researchers think the technique stimulates neurons that initiate movement. Others say it blocks inhibitory neurons, allowing brain signals to resume. And yet another theory holds that it influences the flow of information along axons — fibers that connect neurons to each other.
A recent study published in Science shows that deep brain stimulation exerts its effect on axons, specifically those that feed into the subthalamic nucleus, rather than on the neurons in the structure.
This is the experiment:
For the Science study, the team genetically engineered mice that have a condition that mimics Parkinson’s disease to produce light-responsive proteins only in certain cells in the brain. Then, the researchers inserted fiber optic threads into the mice’s brains. The team used a pulse of blue laser light to increase activity of the cells, or a burst of yellow laser light to quiet the cells. The scientists also used electrical probes to measure activity of the neurons.
When the researchers turned on the light in cells in the subthalamic nucleus nothing happened. But light stimulation of incoming axons improved the mice’s movements. Quieting activity of the axons made the movement disorder worse.
These findings sugests that to stimulate parts of the brain closer to the surface might be an alternative to deep brain surgery. This is a less invasive procedure than DBS.
In yet another Science publication the stimulation of the spinal cord in mice and rats could restore movement to rats and mice with Parkinson’s–like problems.
It’s good news for patients,” says Feng, who was not involved in either study. “Of course, it is not a cure.”
He says that the light-responsive techniques may help uncover the neural circuitry that leads to other psychiatric diseases, such as depression and obsessive-compulsive disorder, which are also sometimes treated with brain stimulation. And spinal cord stimulation or other minimally invasive therapies may offer psychiatric patients an alternative to deep brain surgery.
This will be continued but it will not stop the use of DBS for Parkinson’s disease and why should it, we don’t know how antidepressants work or ECT for that matter.
Thanks Science News
![]()
Gradinaru, V., Mogri, M., Thompson, K., Henderson, J., & Deisseroth, K. (2009). Optical Deconstruction of Parkinsonian Neural Circuitry Science DOI: 10.1126/science.1167093
Fuentes, R., Petersson, P., Siesser, W., Caron, M., & Nicolelis, M. (2009). Spinal Cord Stimulation Restores Locomotion in Animal Models of Parkinson’s Disease Science, 323 (5921), 1578-1582 DOI: 10.1126/science.1164901


 Flickr
Flickr Twitter
Twitter RSS
RSS LinkedIn
LinkedIn GoodReads
GoodReads Last
Last