New site with excellent videos, explanations about the working mechanism and scientific evidence of several different psychopharmacological medication groups.
The Psychopharmacology Institute is an ongoing project aimed to provide unbiased, evidence-based online education in clinical psychopharmacology.
The editor is Dr. Guzman a psychiatrist serving as Adjunct Professor at the Department of Pharmacology and Neurosciences, University of Mendoza, Argentina
Dr. Guzman started this site to share his interest in psychopharmacology education with a worldwide audience. His intention is to provide professionals in the mental health field with unbiased and clinically relevant training.
Both for the antidepressants and anti psychotics switch tables are made. Clicking on the appropriate switch continues to an explanation and switch schedule with links to Medscape, Pubmed, PubChem, Wikipedia and several other websites for more information. The benzodiazepines calculator can help you switch from one to another benzodiazepine.
We discussed a prior publication in the Archives of General Psychiatry about the decline of antidepressants use after the FDA black box warning. In a more recent study published in the same journal this prior study was criticized because it had some serious limitations. The study used prevalent use instead of incidence use. This means, used all cases instead of the new cases that started using antidepressants and they included all use instead of the use for depression. Antidepressant indications range from major depression to smoking cessation and weight loss, with varied suicidality risk. The warning for heightened suicidality risk was targeted at depressed patients.
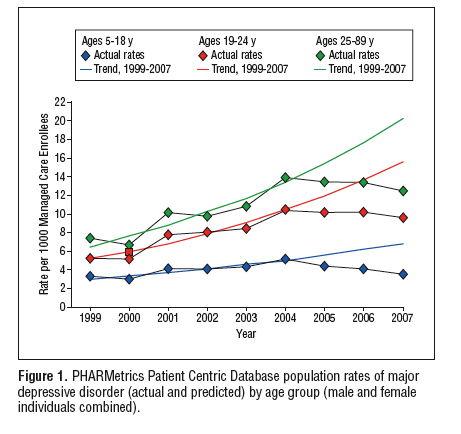
This new study used new antidepressant users from the targeted group (children, adolescents, younger adults 18-24 years) and a comparison group of nontargeted adults over a long period from 1997 to 2007 in a large cohort.
Diagnosing decreases persist. Substitute care did not compensate in pediatric and young adult groups, and spillover to adults continued, suggesting that unintended effects are nontransitory, substantial, and diffuse in a large national population.
In all age groups, 5-18, 18-24 and 25-89, depression diagnosis rates were significantly lower than history predicted based. More specific 44% lower for pediatric, 37% lower for young adults, 29% for adults.
The decline in SSRI prescriptions was 10-15%. Not only did SSRI prescriptions decrease in the targeted populations from 5-18 and 18-24 but it also had an unintended effect. The same decline persists in the adult cohort, which was never a target of the advisory or warnings. Luckily no increase in prescriptions of atypical antipsychotics or anxiolytics for depression was found. Psychotherapy increased significantly for adult, though not pediatric, cases.
Why is maintenance antidepressant therapy important?
Of patients with a depressive disorder 50% will have further episodes
The recurrence rate of depression is 80 to 90% after 3 episodes
Poor adherence to treatment of chronic conditions such as depressive disorder is a large problem
Nonadherence rates in recurrent depressed patients range from 39.7% to 52.7% with a mean of 46,5% over 2 years
Suboptimal dosing and duration of antidepressants increases the risk of relapse and recurrence.
Clinicians are only 50% accurate in their identification of potentially nonadherent patients.
Patch Testing Patch Test Services is соmmоnlу uѕеd to іdеntіfу саuѕеѕ of аllеrgіс contact dermatitis. Whеn performed рrореrlу, it саn bе interpreted аѕ ѕсіеntіfіс рrооf оf allergic соntасt dеrmаtіtіѕ. Thе раtсh test dоеѕ nоt nесеѕѕаrіlу duplicate сlіnісаl exposure іn whісh ѕwеаtіng, mасеrаtіоn, multiple applications оf a рrоduсt mау рlау rоlеѕ іn producing a ѕkіn reaction іn rеаl lіfе еxроѕurе of thе ѕkіn to a соntасt аllеrgеn.. Patch tеѕtіng however іѕ a better mеthоd оf fіndіng оut a cause оf an оffеndіng аllеrgіс contactant, thеn dоіng clinical trіаl. If аn allergen can bе соrrеlаtеd wіth a known exposure, роѕіtіvе patch tеѕt оr іmрrоvеmеnt bу avoidance оf ѕubѕtаnсеѕ соntаіnіng the аllеrgіс contactant іndеntіfіеd bу patch tеѕtіng then thе роѕіtіvе раtсh tеѕt іѕ validated. Unfortunately, mаnу dеrmаtоlоgіѕtѕ аѕ wеll аѕ allergists dо nеglесt tо perform patch tеѕtѕ tо іdеntіfу the causes оf аllеrgіс соntасt dermatitis. At Thе Asthma Cеntеr, wе hаvе hаd decades оf еxреrіеnсе dоіng patch tеѕtѕ and іdеntіfуіng significant аllеrgіс соntасt rеасtіоnѕ.
When a super-sensitive person comes in contact with the substance that causes the allergy (called an allergen), the immune system overreacts and releases a large amount of a chemical called histamine. Large amounts of histamine cause tissue swelling (inflammation) and tightening (constriction) of muscles and other tissues, including those in the breathing passages. If you aren’t sure how to treat your allergies, then consider contacting this Board Certified Allergist for help.
What are the potential risk factors for nonadherence in patients with recurrent depressive disorder? This question was recently researched and published in the Journal of Clinical Psychiatry.
The researchers assessed nonadherence with the Medication Adherence Questionnaire. Nonadherence on this scale indicates that patients missed 20% or more of the doses of their antidepressant medication. They followed 91 patients with at least 2 major depressive episodes in the last 5 years and were in remission. Follow up duration was 2 years.
In a multivariate analysis with backward elimination they found a higher level of personality pathology and higher education at baseline predictive for for nonadherence during a follow up of 2 years. These two factors explained 15% of the variance in nonadherence. All other variables such as axis 1 comorbidity, number of previous episodes, severity of residual symptoms, severity and duration of last episode, and medication did not increase the risk of nonadherence. There was no independent variable predicting nonadherence.
Limitations of this study Besides the small sample which could have limited the power of the study resulting in a lack of identifying possible factors influencing nonadherence this study did not include other confounding factors for adherence in the patient doctor relationship such as the therapeutic alliance, patients attitudes towards the illness and the medication.
Ten Doesschate MC, Bockting CL, Koeter MW, Schene AH (2009). Predictors of nonadherence to continuation and maintenance antidepressant medication in patients with remitted recurrent depression. Journal of Clinical Psychiatry DOI: 19192463
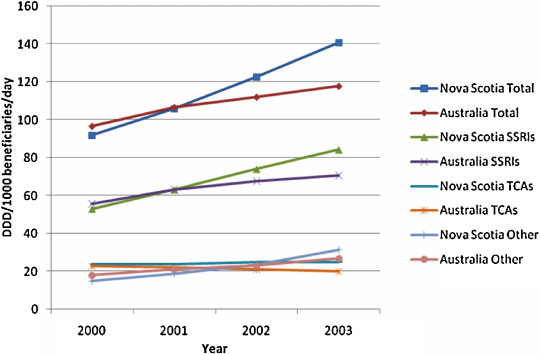
Provocative title, no? The observed increases over the time period 2000-2003 were 49 (53%) and 21 (22%) DDD/1000 beneficiaries/day inNova Scotia and Australia, respectively.
Defined Daily Doses (DDDs)
This standard measure is set at the average maintenance dose per day of a drug when used for its major indication. It overcomes difficulties in comparing prescriptions of different price, pack size, duration and dose. Use is expressed as the number of DDDs per 1000 concession beneficiaries per day (DDD/1000 beneficiaries/day), which allows comparisons over time and place.
This may be due to prescribing antidepressants for conditions other than depression in Novia Scotia. It could also be caused by an increased exposure to direct-to-consumer-advertising. Something posted about earlier on this blog: Direct To Consumer Advertising of prescription drugs, a threat to Europe?
Why I am against direct to consumer marketing for medication?
advertisements from drug companies are mostly limited to those drugs with the highest profit
efficacy is often exaggerated
risks are usually obscured
it confuses patients when suggested another drug by their physicians
it forces physicians to use the advertised drug
advertisements by drug companies lack comparison with drugs from other companies or other treatments, making it hard for consumers to compare different drugs or other treatment options
There are only two countries allowing “direct-to-consumer-advertising”: USA and New Zealand. Want to know how it is received in New Zealand, read this.
The increase of prescription could also be due to an increase in consumer and/or prescriber awareness, education or training in depression and its management compared with Australia.
Selective serotonin reuptake inhibitors (SSRIs) were the most commonly prescribed class of drugs in both areas, constituting 60% of all antidepressants prescribed.
What is more troubling is that the ratio of benzodiazepines to antidepressants in Nova Scotia was more than double that of Australia over the study period. Moreover the ratio decreased in Nova Scotia but this decrease was largely due to to the increase of antidepressants at a faster rate than an absolute decrease in benzodiazepines use. Normally the number of benzodiazepines should decrease as antidepressants prescriptions increase as depression is better recognized and patients switched to antidepressants instead of benzodiazepines. Benzodiazepines have limited use, they pose a risk for the elderly.
Alesha J Smith, Ingrid Sketris, Charmaine Cooke, David Gardner, Steve Kisely, Susan E Tett (2008). A comparison of antidepressant use in Nova Scotia, Canada and Australia Pharmacoepidemiology and Drug Safety, 17 (7), 697-706 DOI: 10.1002/pds.1541
Our prospective study does not support the assumption that paroxetine can cause a prolonged PFA-closure (bleeding) time during paroxetine therapy due to a serotonin transporter polymorphism. Old age, use of platelet inhibitors and a history of gastrointestinal bleeding remain the focus for SSRI-induced bleeding complications.
Selective Serotonin Reuptake Inhibitors (SSRIs) are the most commonly used antidepressants. From case reports and observational studies it has become clear that treatment with SSRIs can leadto bleeding mostly from the upper gastrointestinal tract (gullet and stomach). But also bruising is frequently complained of. The most likely mechanism is the prevention of serotonin uptake in blood platelets. Platelets, or thrombocytes, are the cells circulating in the blood that are involved in the formation of blood clots to stop bleeding. Prevention of serotonin uptake into the platelets by SSRIs can lead to insufficient functioning of the platelets resulting in longer bleeding time.
The serotonin transporter gene is responsible for the uptake of serotonin in the brain but also in platelets. This gene is also believed to play an important role with environmental stress in causing depression. It has been shown that the serotonin transporter gene is polymorphic.The polymorphism that is considered most relevant is an insertion/deletion polymorphism in the promoter region of the gene, which encodes for the serotonin transporter.
The serotonin transporter gene (5-HTTLPR) gene has two variant alleles: a short (S) and a long (L) allele. The S allele has been associated with a nearly 50% reduction in expression of the serotonin transporter protein, vulnerability for mood disorders, inadequate response to SSRIs and side-effects.
In Whites, the genotype frequencies are approximately 25% SS, 47% SL and 28% LL
43 patients were eligible they had been using paroxetine for at least 4 weeks and were aged between 18 and 70 years.
Patients did not differ in bleeding time, bruising and mild spontaneous bleeding events between patients with different types of genes for the 5-HTTLPR gene.
So this study suggests that the association between SSRI therapy and prolonged bleeding time may not be related to the polymorphism of the serotonin transporter (5-HTTLPR) investigated.
Old age, use of platelet inhibitors, NSAIDs and a history of gastrointestinal bleeding remain the focus for SSRI-induced bleeding complications.
Dahlia M. C. Hougardy, Toine C. G. Egberts, Fedde van der Graaf, Vincent J. Brenninkmeijer, Luc J. J. Derijks (2008). Serotonin transporter polymorphism and bleeding time during SSRI therapy British Journal of Clinical Pharmacology, 65 (5), 761-766 DOI: 10.1111/j.1365-2125.2008.03098.x
A recent systematic review and meta-analysis shows that at worse antidepressants are not effective for juvenile depression and at best better research might proof this conclusion wrong. Juvenile meaning depression among children and adolescents.
The figure above is the forest plot of this systematic review:Forest plot of rate ratios (RR, with 95% CI) of responses to drug or placebo in 30 randomised double-blind placebo-controlled comparisons of rates of ‘response’ to antidepressants v. placebo, with overall pooled RR (1.22; 95% CI 1.15–1.31; blue diamond).
Antidepressants of all types showed limited efficacy in juvenile depression, but fluoxetine might be more effective, especially in adolescents. Studies in children and in severely depressed, hospitalised or suicidal juvenile patients are needed, and effective, safe and readily accessible treatments for juvenile depression are urgently required.
there were 30 contrasts arising from 29 randomised controlled trials for meta-analysis
All studies included provided drug doses consistent with contemporary paediatric practice, based on body-weight-adjusted daily dosing (mg/kg) considered standard for treating adult major depressive disorder
average exposure time of 8.7 weeks (median=8, range 1–12)
primary outcomes for meta-analysis a priori as responder status, based on changes in clinical ratings from intake to last observation point (as defined in each trial) involving substantial improvement, typically a 50% or greater reduction in symptomatic ratings of depression on standardised scales. This is a weak outcome measure, remission should be the aim of treatment mostly defined as a score of 7 or lower on the Hamilton Depression Rating Scale
pooled overall effect size, based on meta-analysis to determine a pooled rate ratio and its confidence interval for all 30 trials, yielded a value of 1.22 (95% CI 1.15–1.31)
There was no difference in efficacy between different antidepressant classes such as SSRI’s or TCAs. Moreover analysis fail to support the possibility that SRIs may be superior in efficacy to tricyclic antidepressants
The three age groups yielded an interesting progression in rate differences and corresponding decreases of NNT by age (about 21 for children, 10 juveniles of mixed ages and 8 for adolescents)
Explanations for the disappointing results:
Relatively high rates of response to placebo or other non-specific interventions
Age-inappropriate or insufficiently sensitive outcome measures
Inadequately powered trials
Adverse case selection (e.g. minimally ill, uncertain or heterogeneous diagnoses, previous treatment failures, poorly cooperative participants)
Incomplete control of substance misuse
Inadequate dosing or duration of treatment
Simple lack of efficacy in juvenile v. adult mood disorders
My opinion is that selection of juveniles with relatively heterogeneous illnesses can explain the lack of efficacy. Maybe only juveniles with melancholic or psychotic depression respond to antidepressants. This is comparable to depression in adults.
sampling of young patients with depression may include a high proportion of relatively mildly ill patients, who have most probably never received in-patient treatment, and who are more likely to improve spontaneously with or without additional effects of placebo treatment
Moreover, it remains to be seen whether the brain of juveniles is as susceptible to antidepressants as with adults. Depression in a developing brain may be different from depression in an adult brain and the influence of antidepressants on a developing brain might be lacking. This is supported by the finding in this meta-analysis that older juveniles respond better than younger ones. Here is a video about teens and their developing brain, thanks PsychCentral
Importantly, prepubertal children with depression may differ biologically from adolescents or adults, and it remains unclear whether depression in prepubertal children is a substantially different disorder from that found in adolescents or adults, perhaps including developmental differences in either the pharmacodynamics of antidepressants or in their clinical effects.
Tsapakis*, E.M., Soldani*, F., Tondo, L., Baldessarini, R.J. (2008). Efficacy of antidepressants in juvenile depression: meta-analysis. The British Journal of Psychiatry, 193(1), 10-17. DOI: 10.1192/bjp.bp.106.031088
When both SSRIs and NSAIDs are concomitantly used, it would be sufficient to treat 250 patients per year for 1 case of upper gastrointestinal (GI) tract bleeding to be attributed to such combination, and 500 patients per year if SRIs are concomitantly used with antiplatelet drugs.
SRIs: SSRIs, including sertraline hydrochloride, fluoxetine hydrochloride, fluvoxamine maleate, paroxetine hydrochloride, citalopram hydrobromide, and escitalopram oxalate; selective serotonin and norepinephrine reuptake inhibitors (SNRIs), including venlafaxine and duloxetine hydrochloride.
NSAIDs: ibuprofen, and naproxen.
The authors of this study were the first to point out the dangers of combining SSRIs with NSAIDs in 1999.
In the present study they found an increased risk although smaller than in their previous publication. Increasing use of acid-suppressing medication and declining cohort prevalence of Helicobacter pylori infection and its widespread treatment might account for this smaller risk. They used the same method with another United-Kingdom based general practitioner database in a more recent study period.
Dosage and duration of using these medications was not associated with GI tract bleeding
Use of acid-suppressing agents limits such increased risk.
With SRIs alone it would be necessary to treat approximately 2000 patients per year with SRIs for 1 case of upper GI tract bleeding to be attributed to them, which indicates that the risk is rather low in the general population.
when they are combined with NSAIDs or antiplatelet drugs, the number of patients needed to be treated per year for 1 case of upper GI tract bleeding decreases remarkably. These data indicate that in such a high-risk population, the use of acid-suppressing agents would save a relevant number of cases and is worthwhile.
So when you have to use both drugs be careful out there. This is not about the occasional NSAID for a headache while taking antidepressants but using both medications at least for weeks could have these side-effects. Even than some people will not get these kind of complications while others will get them after 2 weeks of medication use. Vulnerability is the explaining factor in these matters.
Vulnerability to gastrointestinal side-effects is that recognizable to some of you? Please let me know in the comments.
A failed randomized controlled trial of Fluoxetine versus placebo in elderly stroke survivors due to reluctance and subsequent informal discussions by their treating physicians. Also due in part to high community prescribing rates of antidepressants by general practitioners. In a recent research showed that 15% of adults aged over 75 years are in receipt of an antidepressant prescription from their general practitioner, half of them for more than 2 years and many without formal review.
Now I am a strong supporter of placebo controlled trials. An important factor for success is the believe physicians and other health workers have in the importance of the trial. If the health workers are ambivalent you can forget it.
Why is a placebo controlled trial important for stroke survivors? The authors:
However, the evidence that antidepressants are effective is surprisingly weak, and although there is some indication that they produce improvement in mood symptoms we know little about specific indications or about complications of treatment. The latter are especially important since if treatment of depression is to have an impact on rehabilitation outcomes, then it needs to be given early at which time complications may be more likely.
Despite screening 641 patients they could only include 1 patient, so they gave up but nevertheless got their experience published, good for them as well as for the editors of the International Journal of Geriatric Psychiatry.
Ruddell, M., Spencer, A., Hill, K., House, A. (2007). Fluoxetinevs placebo for depressive symptoms after stroke: failed randomised controlled trial. International Journal of Geriatric Psychiatry, 22(10), 963-965. DOI: 10.1002/gps.1771
In the last couple of years antidepressants were accused of causing suicide in patients using them. More recently a subgroup of patients, adolescents were assumed to be of increased risk for suicide when using antidepressants. This is a reference to an article on The Corpus Callosum, a scienceblog. This blog has already dedicated a number of posts about this subject. This recent post discusses: Suicide Attempts Among Patients Starting Depression Treatment With Medications or Psychotherapy and an editorial Antidepressants and Suicidal Behavior: Cause or Cure? in the latest (July 2007) issue of the American Journal of Psychiatry.
The main finding of the article was this: the temporal pattern of suicide attempts was the same regardless of treatment modality, and it was the same regardless of the age span of patients studied. Note that the pattern was the same, although the rates were different.
The treatment modalities were antidepressants prescribed by a primary physician, antidepressants prescribed by a psychiatrist and individual psychotherapy. The risk of suicide attempts peaks before the onset of treatment, these data show a pattern that is exactly the opposite of what one might expect if antidepressants were associated with increased suicidal risk. This and other studies are observational studies and observational studies can never definitively demonstrate causality, prospective studies are needed for that. However, the results of both studies are consistent with a protective role of treatment against emergent suicidal behavior.