Why some people don’t like the humor of Monthy Python

This image above shows two types of humor. One based on incongruity-resolution, the cartoon on the left. The other also based on incongruity-resolution but provoked by a nonsense cartoon on the right.
Humor of nonsense jokes and cartoons is a different sense of humor according to recent research. Not in the sense of the neural processing of humor in the brain or to their structural properties but they differ in content.
The common element of these humorous stimuli is that in their processing the recipient first discovers an incongruity. This incongruity can be easily resolved upon reinterpretation of the information available in the joke or cartoon. The cartoon on the left. Or on the other end of the spectrum, the cartoon on the right it can’t be easily resolved. It’s complete nonsense. The cartoon doesn’t provide a resolution at all. Or it provides a very partial resolution (leaving an essential part of the incongruity unresolved), or actually create new absurdities or incongruities.
It’s the difference between people who like the utter nonsense of Monthy Python and those who don’t. It’s the difference between your comic TV show and Monthy Python’s Flying Circus.
This appreciation of nonsense jokes and cartoons is dependable on personality characteristics. Those with a high level of experience seeking appreciate nonsense humor more.
Experience seeking involves a search for novel sensations,
stimulation and experiences through the mind and senses, through
art, travel, music, and the desire to live in an unconventional style
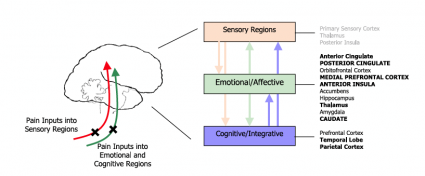
With fMRI scans it was shown that for incongruity resolution as compared to this resolution for nonsense cartoons the former had more activation of brain structures necessary with the processing of humor. These brain structures being the anterior medial prefrontal cortex, bilateral superior frontal gyri and temporo-parietal junctions (TPJ). These brain structures show more activation during processing of incongruity-resolution than of nonsense cartoons.
![]()
Samson, A., Hempelmann, C., Huber, O., & Zysset, S. (2009). Neural substrates of incongruity-resolution and nonsense humor Neuropsychologia, 47 (4), 1023-1033 DOI: 10.1016/j.neuropsychologia.2008.10.028